 **For information about AMRPA's Summer 2024 Prior Authorization Survey, please click here.**
**For information about AMRPA's Summer 2024 Prior Authorization Survey, please click here.**
Access to Inpatient Rehabilitation for Medicare Advantage Beneficiaries: An Examination of Prior Authorization Practices
Download PDF Version of this Report
Read AMRPA Response to CMS Request for Information on Prior Authorization
Abstract:
The use of prior authorization (PA) by Medicare Advantage (MA) plans is a pressing concern among rehabilitation providers. A nationwide survey of rehabilitation hospitals and units (RHUs) was conducted to determine how frequently PA was used to deny admission to an RHU, how timely those decisions were rendered, and the resulting consequences for patients. The survey, which tracked data for one month (August 2021), found that MA plans overrule rehabilitation physician judgment at a rate of 53%. In addition, patients wait on average more than two and half days for a determination. This resulted in more than 30,000 days waiting for determinations during the single survey month. Since the vast majority of patients being referred to an RHU are hospitalized in an acute hospital, enormous cost and burden results from the use of PA. In addition, seriously impaired MA beneficiaries may be harmed by denials and delays in access to care.
Introduction and Background
Medicare Advantage (MA) plans offer various premium and cost-sharing arrangements that differ from traditional Medicare (TM), as well as health and wellness benefits not offered to beneficiaries enrolled in TM. In addition to financial flexibilities, MA plans are permitted to employ various utilization management strategies not regularly used in TM, including requiring prior authorization (PA) of an item or service as a condition of payment. When PA is required by MA plans, the plan must pre-approve the service, or payment will not be made to the provider. While the use of PA to manage benefits is permitted, MA plans are nonetheless obligated by law to provide all of the benefits offered in TM.
The number of beneficiaries who have chosen to enroll in MA plans has grown at an accelerated pace in recent years. Of the approximately 64 million Medicare beneficiaries, an estimated 28 million now receive their Medicare benefits through private insurers that have contracted with CMS to offer MA plans.
As enrollment in MA has grown, providers have reported that PA determinations and subsequent denials have increased and often do not follow appropriate evidence-based guidelines. In addition, physicians report the PA process often delays care and has a negative impact on clinical outcomes. Concerns have also been raised about the lack of accountability for the use of PA by MA plans. These concerns are due to high overturn rates of denials and due to insufficient publicly reported data.
In the context of rehabilitation hospitals and units (RHUs), PA delays the discharge of patients from an acute hospital, and denies or delays access to needed therapeutic interventions. RHUs (referred to by Medicare as Inpatient Rehabilitation Facilities or IRFs) provide specialized physician-directed care that includes close medical management and an intensive program of rehabilitation. The goals of care in a RHU include continuing medical management of the patient’s underlying health problems and improving the patient’s functional capacity so that the patient can return to the community. The vast majority of patients referred for admission to an RHU are in an acute hospital due to serious illness or injury.
The Medicare coverage criteria stipulate that a RHU stay is eligible for payment if the patient would practically benefit from and tolerate intensive, multi-disciplinary therapy and requires ongoing supervision by a rehabilitation physician. The Medicare rules also require that a rehabilitation physician approve each patient for admission. Due to the stringent Medicare rules and the intensity of services offered, RHUs treat more seriously ill and functionally impaired patients than lower intensity post-acute care settings.
Medicare does not have regulatory requirements for PA response times that are specific to hospitalized patients. This has increasingly become a concern since many providers have reported exacerbation of the process burden and high rates of denials for PA requests for admissions. In addition, there is essentially no publicly available data to determine the consequences of PA requirements at the initial determination level or at the initial appeal level. Medicare and its contractors do report the outcomes of the second level of appeal (formally referred to as “Reconsideration by an Independent Review Entity”). However, this level of appeal is rarely utilized for patients seeking admission to an RHU given the lengthy and time-consuming process, which is impractical for patients in need of immediate care decisions.
Given the lack of available data on PA practices and outcomes, the American Medical Rehabilitation Providers Association (AMRPA) conducted a survey of RHUs across the nation to gain more quantitative and qualitative information, including the pervasiveness of PA use as a benefits management practice, frequency of denials, and associated delays in care.
Survey Objectives
The goals of this survey were to determine how common denials of authorization for RHU care are, how timely those determinations are made, and what the consequences of those determinations may be.
Design
RHUs were solicited to participate prospectively in a data collection effort for the month of August 2021. The survey was publicized through trade association and professional channels to the RHU community, including disclosure of the specific questions that would be included on the survey and a spreadsheet form that could be used to capture the PA activity as it occurred. Participants submitted their data via an online portal.
The survey consisted of nine questions, shown below in Table 1.
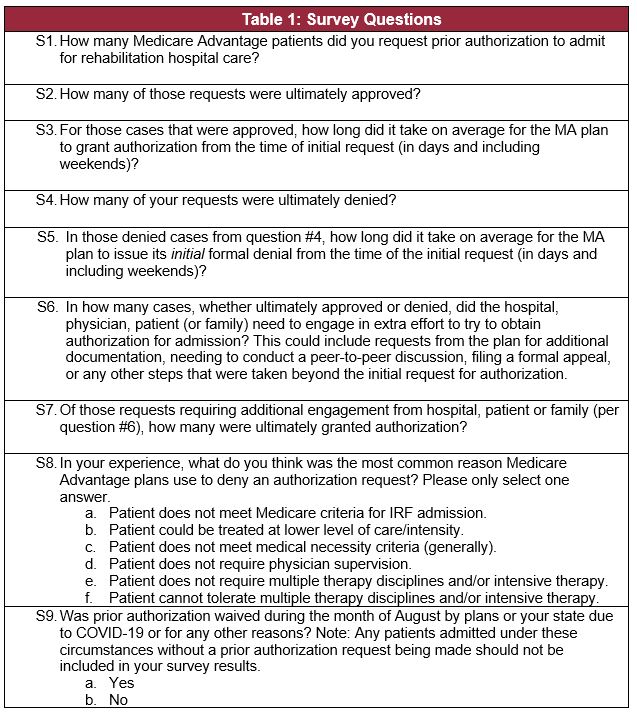
Participants
Data were submitted by 102 respondents who provided information about a total of 475 RHUs, representing approximately 40% of the RHUs nationwide. The responses included RHUs from 47 states and Puerto Rico. Data on 12,157 PA requests for the month of August 2021 were included in the survey.
Results
Of the 12,157 PA requests reported for the month, 6,482 of those requests were initially denied by the MA plan (53.32% of all requests). 84% of respondents reported that 30-70% of initial requests were denied during the survey month. Figure 1 shows the distribution of denial frequency cited by RHUs.
Figure 1. Distribution of Hospitals by denials

Wait times of greater than 2 days for requests were typical for the vast majority of respondents, with 84% of respondents waiting more than 2 days on average for all requests. The average wait time for the initially approved requests was 2.49 days. The average wait time for the initially denied requests was 2.59 days.
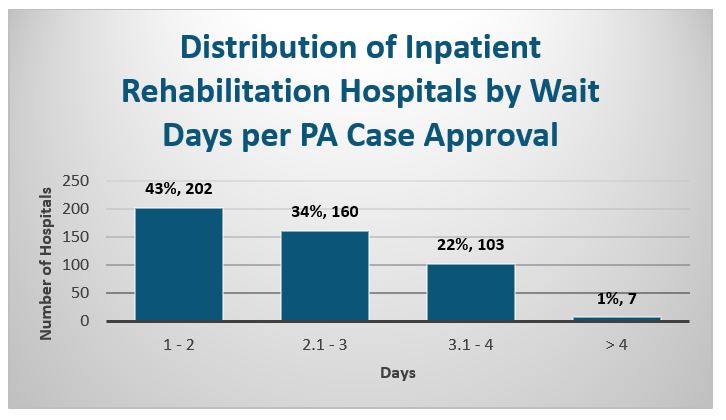
The wait times were very consistent across all IRFs. 84% of RHUs also reported an average wait time of 2.1 days or greater for denied requests. For approved requests, the majority (56%) had wait periods over two days. Figure 2 shows the distribution of wait time for a negative response. Figure 3 shows delays experienced when an initial favorable response was received.
Figure 2. Distribution of Hospitals by wait time for negative response
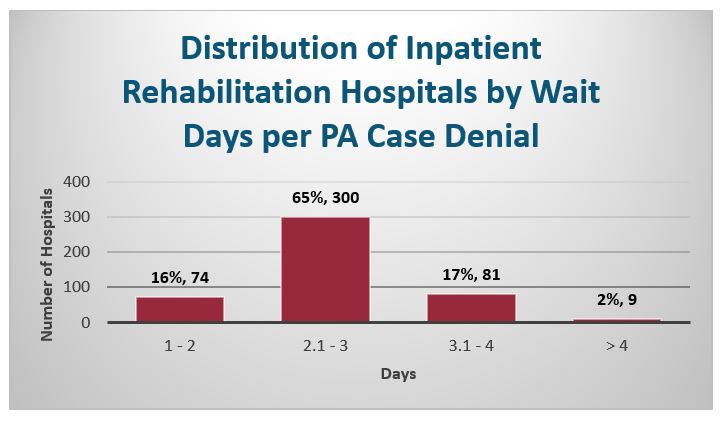
Figure 3. Distribution of Hospitals by wait time for favorable response
A total of 14,152 acute hospital days were spent waiting for requests that were ultimately approved, and 16,774 acute hospital days were spent waiting for denied requests, totaling 30,926 total acute hospital days spent waiting for a determination.
Respondents provided information regarding any additional effort required to seek authorization for 4,823 requests. 35.39% of these requests required additional effort on behalf of the hospital, physician, patient or family. For requests that required this additional effort, 28.94% were approved for admission as part of the initial request.
The most commonly provided reason for a denial cited by RHUs was that the patient “could be treated at a lower level of care/intensity.” The next most common reason was that the patient “does not meet medical necessity criteria.” Some respondents indicated multiple rationales for denying payment so the total of reasons reported exceeds 100%. Finally, 29% (136) of respondents indicated that PA was waived at some point during the survey month by plans or regulators due to the COVID-19 pandemic.
Discussion
PA is being commonly used to deny patient access to RHU care. These determinations are difficult to challenge, since subsequent appeals take additional days, and the patient typically must be transferred more promptly than that. The data presented here shows that even when a MA plan agrees with the request, there are substantial delays in communicating that decision. With these delays and denials, there is an associated risk that patients may be harmed.
The high frequency of denials suggests that there is a striking disagreement between the medical decisions of practicing rehabilitation physicians and the judgments being rendered by MA plans. Since rehabilitation physicians determined that each of these referred patients required RHU admission, the widespread denials by MA plans calls into question what criteria and expertise plans utilized to render decisions.
Although MA plans are not required to disclose the specific expertise and guidelines they use to reach determinations, respondents reported the primary reason cited for a denied request was that the patient “could be treated at a lower intensity setting of care.” This is disconcerting because Medicare has stated that this shall not be a basis for denying RHU coverage, yet denials for this reason appears to be a common practice by MA plans. Whether a patient could be treated elsewhere is not one of the Medicare criteria used by physicians to determine whether the patient is appropriate for inpatient rehabilitation admission. Instead, that determination is made based on whether the patient meets the enumerated Medicare standards, referenced above. This finding is consistent with other surveys that have found that plans utilize improper medical guidelines for PA requests.
If any of the denied patients been enrolled in TM, they likely would have been admitted to the RHU without delay. Instead, because the beneficiary chose to enroll in MA, and due to the opaque review process and criteria utilized by MA plans, the patients were denied access to the RHU.
Medicare regulations require MA plans to issue determinations “as expeditiously as the enrollee's health condition requires, but no later than 72 hours after receiving the request.” This survey shows that MA plans consistently do not issue determinations as expeditiously as the beneficiary’s condition requires, since such a response would be made within minutes to hours, not days. It is likely that in many cases, PA unduly delays the initiation of needed therapeutic interventions and hampers patients’ recovery. This finding is again consistent with other surveys that indicate PA detrimentally impacts clinical outcomes for patients.
The data presented here represent only one month of activity during the COVID-19 Pandemic and National Public Health Emergency. Since the vast majority of patients seeking admission to an RHU are hospitalized in an acute hospital, each day of delay in transfer represents increased risk and cost. Since MA plans typically pay for hospital admissions on a prospective basis, the immediate additional cost is borne by the hospital. As these additional lengths of stay are captured through Medicare’s tracking of resource utilization, payments may be increased due to extended length of stay for these patients, costing Medicare additional unnecessary dollars.
Conclusions
MA plans’ use of the PA process to delay and deny patient transfers of from acute hospitals to RHUs is a widespread and common problem that can harm patients. PA processes increase administrative burden, delay necessary care, and increase waste and cost to the health care system.
There is an urgent need to eliminate these unnecessary delays in providing care to patients and mitigate denials based on opaque and inconsistent criteria. These needs can be addressed by regulatory and contractual changes to the MA plan operational requirements, and by ensuring that qualified clinicians are making proper and timely determinations about RHU referrals.
References
1. 42 C.F.R. § 422.101.
2. Bob Herman, Medicare Advantage enrollment soars almost 9%, Axios (Jan. 18, 2022), https://www.axios.com/medicare-advantage-enrollment-2022-soars-055b6d7d-d2c7-4e69-9eba-420c0ee4ef6e.html.
3. American Medical Association, 2020 AMA Prior Authorization (PA) Physician Survey, (April, 2021) https://www.ama-assn.org/system/files/2021-04/prior-authorization-survey.pdf & https://www.ama-assn.org/system/files/2021-05/prior-authorization-reform-progress-update.pdf.
4. American Medical Association, 2021 AMA Prior Authorization (PA) Physician Survey, (February, 2022) https://www.ama-assn.org/system/files/prior-authorization-survey.pdf
5. HHS Office of Inspector General (OIG), Medicare Advantage Appeal Outcomes and Audit Findings Raise Concerns About Service and Payment Denials (Sept. 25, 2018) (https://oig.hhs.gov/oei/reports/oei-09-16-00410.asp).
6. 42 C.F.R. 412.622.
7. CMS Inpatient Rehabilitation Facility Data, General Information Data Set (December 2021), https://data.cms.gov/provider-data/topics/inpatient-rehabilitation-facilities.
8. Assessment of Patient Outcomes of Rehabilitative Care Provided in Inpatient Rehabilitation Facilities (IRFs) and After Discharge; Dobson & Davanzo (July 2014) (https://amrpa.org/Portals/0/Dobson%20DaVanzo%20Final%20Report%20-%20Patient%20Outcomes%20of%20IRF%20v_%20SNF%20-%207_10_14%20redated.pdf)
9. CMS IRF PPS Coverage Requirements Nov. 12, 2009 National Provider Conference Call (“Notice that nowhere on the slide and nowhere in this presentation are we going to talk about whether the patient could have been treated in a skilled nursing facility or another setting of care. Under the new requirements, a patient meeting all of their required criteria for admission to an IRF would be appropriate for IRF care whether or not he or she could have been treated in a skilled nursing facility.”) (Available for download: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientRehabFacPPS/Coverage).
10. American Medical Association, 2020 AMA Prior Authorization (PA)
11. Physician Survey, (April, 2021) https://www.ama-assn.org/system/files/2021-04/prior-authorization-survey.pdf & https://www.ama-assn.org/system/files/2021-05/prior-authorization-reform-progress-update.pdf.
12. 42 C.F.R. § 422.572(a).
13. American Medical Association, 2020 AMA Prior Authorization (PA)
14. Physician Survey, (April, 2021) https://www.ama-assn.org/system/files/2021-04/prior-authorization-survey.pdf & https://www.ama-assn.org/system/files/2021-05/prior-authorization-reform-progress-update.pdf.
15. Why Medicare Advantage Plans Pay Hospitals Traditional Medicare Prices, Robert A. Berenson, Jonathan H. Sunshine, David Helms, and Emily Lawton, Health Affairs 2015 34:8, 1289-1295 (https://www.healthaffairs.org/doi/10.1377/hlthaff.2014.1427).